
Research article/ Open Access
DOI:10.31488/EJRM.156
Individualized PEEP Titration Guided by Driving Pressure after Recruitment Maneuver Reduces Postoperative Pulmonary Complications in Cardiac Surgery: A Randomized Controlled Trial
Natália Coronel de Lima Lages1,2, Mariana Barcellos de Ávila1,2, Tiago Batista da Costa Xavier2,3, Luciana Moisés Camilo2,3
1. Hospital Universitário Pedro Ernesto (HUPE), Universidade do Estado do Rio de Janeiro (UERJ), Rio de Janeiro, Brazil
2. Instituto de Biofísica Carlos Chagas Filho, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil
3. Instituto Federal de Educação, Ciência e Tecnologia do Rio de Janeiro (IFRJ), Rio de Janeiro, Brazil
*Corresponding author: : Dr. Natália Coronel de Lima Lages, ORCID: [0000-0001-5121-9123],Hospital Universitário Pedro Ernesto, Blvd. 28 de Setembro, 77 - Vila Isabel, Rio de Janeiro - RJ, 20551-030, Tel: +5521997795518; E-mail: nataliacoronellages@gmail.com
Abstract
Background: Postoperative pulmonary complications (PPCs) are a frequent cause of morbidity following cardiac surgery. The use of individualized mechanical ventilation strategies, particularly those based on driving pressure (dP), may improve pulmonary outcomes compared with fixed positive end-expiratory pressure (PEEP) protocols. Objective: To evaluate whether PEEP titration guided by the lowest dP after an alveolar recruitment maneuver (ARM) reduces the incidence of clinically significant PPCs in patients undergoing elective cardiac surgery. Design: Prospective randomized controlled trial. Setting: Cardiac surgery ICU of a tertiary university hospital (July 2021–October 2023). Participants: Adults undergoing elective cardiac surgery with cardiopulmonary bypass. Intervention: Recruitment maneuver followed by decremental PEEP titration to lowest dP versus fixed PEEP 10 cmH₂O. Main Outcome: PPC ≥ grade 3. PPCs were classified according to the modified Kroenke score (grades 0–5). Results: One hundred patients were randomized and 97 analyzed. PPC ≥3 occurred in 40.8% of controls and 12.5% of the intervention group (absolute risk reduction 28.3%, p = 0.002). Pneumonia incidence was 28.6% vs 8.3% (p = 0.010). Driving pressure (dP) decreased significantly (6 vs 8 cmH₂O, p < 0.001) with improved oxygenation and compliance. No increase in adverse events was observed. Conclusion: Driving pressure–guided individualized PEEP significantly reduces severe PPCs after cardiac surgery without compromising hemodynamic stability.
Keywords: Driving pressure, PEEP, cardiac surgery, postoperative pulmonary complications, recruitment maneuver
Introduction
Cardiac surgery is associated with several postoperative pulmonary complications (PPCs), with atelectasis being the most prevalent, occurring in 30–72% of cases, and pleural effusions in 24–63%. Other complications include pneumonia (2–20%), phrenic nerve injury (10–21%), prolonged mechanical ventilation (MV) lasting more than 48 hours (2–6%), and acute respiratory distress syndrome (ARDS) (0.4–2%). These conditions often result in longer hospital stays and increased healthcare costs, highlighting the need for effective preventive and therapeutic strategies in the postoperative management of patients undergoing cardiac surgery [1].
Protective mechanical ventilation is a fundamental strategy to minimize ventilation-induced lung injury. This approach aims to reduce stress and strain on the lungs, preventing complications such as volutrauma and atelectrauma. Biotrauma, in turn, refers to lung injury resulting from the local and systemic inflammatory response triggered by mechanical ventilation-related insults, such as volutrauma and atelectrauma. These mechanisms promote the release of inflammatory mediators, contributing to additional damage to lung tissue [2].
Postoperative pulmonary complications (PPCs) are adverse events that may occur after surgical procedures, ranging from atelectasis to pneumonia, respiratory failure, and exacerbation of pre-existing pulmonary diseases. These complications are associated with increased morbidity, prolonged hospital stay, and higher mortality [2]. Depending on severity, PPCs may range from mild atelectasis to severe conditions such as acute respiratory distress syndrome (ARDS) [3,4].
In the context of cardiac surgery, the expected incidence of complications requiring intervention (PPCs grade ≥ 3) reaches 30%, according to the modified pulmonary complication score by Kroenke et al. [2,5].
Manifestations such as respiratory failure (RF), which occurs in 20–25% of cases, require prolonged MV and longer ICU stays [6] . Several factors contribute to RF, including atelectasis, hyperoxemia with free radical release [7] , and a systemic inflammatory response related to Cardiopulmonary bypass (CPB) [8,9].
CPB itself has been identified as a determining factor for pulmonary atelectasis, being responsible for most intrapulmonary shunt and significant reductions in blood oxygenation. Although thoracic surgery also contributes to pulmonary collapse to a lesser extent, the period of absent ventilation and perfusion during CPB has been highlighted as the main insult. These findings suggest that atelectasis plays a crucial role in gas exchange dysfunction observed after this procedure [10].
Suspension of MV during CPB is widely practiced since oxygenation is achieved by extracorporeal systems. However, this approach is associated with the development of atelectasis and hydrostatic pulmonary edema, resulting in decreased pulmonary compliance [8,9]. These aspects underscore the need to further investigate optimal ventilatory strategies for the immediate postoperative period in these patients.
Evidence indicates that adopting protective ventilation methods can attenuate systemic and pulmonary inflammatory responses in patients undergoing myocardial revascularization [11], as well as improve functional residual capacity (FRC) and oxygen saturation compared to conventional ventilation [12].
Driving pressure (dP) is an additional protective MV variable calculated as the difference between plateau pressure (Pplat) at end-inspiration and PEEP, reflecting the distending pressure exerted on the respiratory system [4,13] . This parameter has been associated with normalized lung strain relative to residual aeration. In ARDS patients, a dP above 15 cmH₂O has been linked to higher mortality, with a 5% increase in death risk for each 1 cmH₂O increment [14-16].
In surgical patients, a meta-analysis [4] demonstrated an association between higher dP values and increased risk of PPCs. In clinical practice, many patients receive MV with high tidal volumes, variable PEEP, and often elevated ΔP during the intraoperative period [17,18].
The use of recruitment maneuvers (ARM) and individualized PEEP aiming to reduce dP with low tidal volume during intraoperative ventilation in surgical patients carries a strong recommendation level according to consensus [19]. A recent meta-analysis in cardiac surgery patients demonstrated that an ARM with 40 cmH₂O can reduce atelectasis, hypoxemic events, and pneumonia, as well as improve the arterial oxygen partial pressure to inspired oxygen fraction ratio (PaO₂/FiO₂), without causing hemodynamic disturbances [20]. In the same study, subgroup analysis revealed that postoperative ARM produced the same beneficial effects as intraoperative ARM, with the added advantage of not interfering with the surgical procedure.
At the University Hospital Pedro Ernesto (HUPE, UERJ), the Cardiac Surgery Unit protocol recommends that patients be ventilated in the immediate postoperative period (IPP) using protective tidal volumes and a fixed PEEP of 10 cmH₂O, without prior ARM. This PEEP level is maintained until the spontaneous breathing trial (SBT), despite recent studies demonstrating that individualizing PEEP based on patient-specific respiratory mechanics can optimize oxygenation and minimize ventilation-associated complications [21-23].
Mechanical ventilation, although essential for ensuring adequate gas exchange, differs substantially from physiological breathing and may induce adverse effects related to lung mechanics and cardiopulmonary interactions. Insufficient end-expiratory lung volume favors alveolar collapse and cyclic recruitment, whereas excessive distending pressures promote overdistension, both contributing to ventilator-induced lung injury through mechanical stress and inflammatory pathways. These mechanical alterations are closely linked to hemodynamic consequences, as positive intrathoracic pressure modifies venous return, ventricular loading conditions, and pulmonary vascular resistance. Consequently, the balance between preventing alveolar collapse and avoiding overdistension is central to optimizing ventilation while preserving cardiovascular function [24].
In this context, the present study evaluated the impact of individualized PEEP adjustment, based on the lowest dP following an alveolar recruitment maneuver, as a strategy to optimize pulmonary protection. The central hypothesis was that this individualized PEEP approach would lead to a greater reduction in PPC incidence compared with fixed-PEEP protocols, positively influencing patient prognosis.
Methods
Study design and ethical approval
A situational diagnosis was previously conducted through a prospective analysis involving 109 patients who underwent cardiac surgery between November 2020 and January 2021.
This preliminary assessment of the incidence of postoperative pulmonary complications (PPCs) in our service was essential to characterize the profile of our patient population and to identify the frequency and severity of these complications.
Regarding complication severity, PPCs with a score ≥3 (Table 1) was analysed. These include severe events such as pneumonia, prolonged non-invasive ventilation, reintubation, invasive mechanical ventilation lasting more than 48 hours, and pleural effusion requiring drainage. Such complications are associated with higher morbidity, prolonged need for ventilatory support, longer ICU and hospital stays, and potential implications for mortality.
Table 1. Classification of Postoperative Pulmonary Complications According to the Modified Kroenke et al. Score (2015).
| Grade | Description |
|---|---|
| Grade 0 | No signs or symptoms. |
| Grade 1 |
• Dry cough. • Microatelectasis: abnormal pulmonary findings and axillary temperature > 37.5°C with no other documented cause, and a normal or unavailable chest radiograph. • Dyspnea with no documented cause. |
| Grade 2 |
• Productive cough with no documented cause. • Bronchospasm resulting in a change of therapy. • Hypoxemia with SpO₂ < 90% on room air associated with dyspnea or wheezing. • Atelectasis confirmed by chest radiograph and axillary temperature > 37.5°C or abnormal pulmonary findings. • Transient hypercapnia (PaCO₂ > 50 mmHg) requiring intervention. |
| Grade 3 |
• Pleural effusion requiring thoracentesis. • Suspected pneumonia with radiological evidence but without bacteriological confirmation. • Confirmed pneumonia with radiological evidence and identification of the causative organism (culture or Gram stain). • Pneumothorax. • Reintubation with mechanical ventilation lasting less than 48 hours. |
| Grade 4 | • Need for reintubation and/or invasive mechanical ventilation for 48 hours or longer. |
| Grade 5 | • Death before hospital discharge. |
PPCs were classified according to a modified ordinal scoring system based on Kroenke et al. (2015), ranging from grade 0 (no pulmonary symptoms) to grade 5 (in-hospital death). The highest grade observed during hospitalization was considered for analysis
This analysis revealed that 32% of patients presented PPCs with a score ≥3, reinforcing the importance of implementing preventive measures and optimizing protective ventilatory support to reduce these complications.
Based on these findings, an alveolar recruitment protocol was developed, incorporating PEEP titration guided by the lowest driving pressure (dP), with the goal of reducing the incidence of such complications to 15%, in accordance with the findings of Costa Leme et al. [2].
Patients were followed daily by a multidisciplinary team composed of physicians, physiotherapists, nurses, nutritionists, and psychologists, and underwent comprehensive clinical evaluation, including laboratory and imaging studies such as ultrasonography, chest radiography, and, when necessary, computed tomography (CT) of the chest. Routine chest radiographs were obtained and analyzed on the first and second postoperative days, as well as on the day of ICU discharge, with additional imaging performed when clinically indicated.
The interpretation of clinical, laboratory, and imaging data, as well as the grading of PPCs during the situational diagnosis phase, was independently performed by two intensive care physiotherapists blinded to patient allocation, with only concordant assessments considered for scoring. The progression of complications was monitored daily until hospital discharge.
This was a prospective, randomized, controlled clinical trial conducted in the cardiac surgery intensive care unit (ICU) at Hospital Universitário Pedro Ernesto (HUPE), Universidade do Estado do Rio de Janeiro, Brazil, between July 2021 and October 2023. The study protocol was approved by the institutional Research Ethics Committee (CAAE: 5041157; approval date: October 15, 2021). All participants or their legal representatives signed informed consent forms prior to inclusion. The study was prospectively registered in the Brazilian Clinical Trials Registry (ReBEC, RBR-2nmwxwt).
Inclusion criteria
Patients aged 18 years or older who provided written informed consent (ICF) were included in the study. Eligible participants were those undergoing elective cardiac surgery involving planned use of cardiopulmonary bypass (CPB), aortic cross-clamping (CLAMP), administration of a cardioplegic solution, and median sternotomy. Additionally, patients were required to have optimized volemia, defined as an inferior vena cava (IVC) diameter greater than 18 mm, and a mean arterial pressure (MAP) above 80 mmHg.
Exclusion criteria
Patients were excluded if they refused to participate, had a history of previous cardiac surgery, pulmonary fibrosis, pulmonary emphysema, or pneumonia diagnosed within the last 30 days. Other exclusion criteria included pulmonary arterial hypertension (PAH) with a systolic pulmonary artery pressure (sPAP) greater than 45 mmHg, need for orotracheal intubation (OTI) prior to arrival in the operating room, obesity with a body mass index (BMI) greater than 40 kg/m², requirement for norepinephrine > 2 μg/kg/min, need for reoperation, pneumothorax and/or presence of active bubbling chest drains, neuromuscular disorders, or undergoing coronary artery bypass grafting (CABG) using the right internal mammary artery (RIMA) or radial artery grafts. Patients who experienced intraoperative complications were also excluded.
Discontinuation criteria
Criteria for discontinuation of the study included hemodynamic instability with norepinephrine requirement greater than 2 μg/kg/min, mean arterial pressure (MAP) below 60 mmHg, occurrence of acute arrhythmias, or a drop in oxygen saturation (SpO₂) below 90%. These parameters indicated immediate interruption of the alveolar recruitment and PEEP titration protocol. Furthermore, a PaO₂/FiO₂ ratio below 150 mmHg after 60 minutes with PEEP of 10 cmH₂O in the control group was defined as a withdrawal criterion, prompting the initiation of an oxygenation rescue maneuver.
Randomization and blinding
Patients were randomized 1:1 using computer-generated allocation. Outcome assessors were blinded to group assignment.
Hemodynamic and respiratory monitoring
Patients were continuously monitored via invasive arterial pressure, electrocardiography, peripheral oxygen saturation (SpO₂), and heart rate. No invasive hemodynamic monitoring (e.g., pulmonary artery catheterization) was performed during the ARM.
Interventions
Control group
Patients in the control group (CG) were admitted to conventional protective mechanical ventilation in the immediate postoperative period (IPP) using the volume-controlled ventilation (VCV) mode, with a tidal volume (VT) of 6 mL/kg of predicted body weight, a PEEP of 5 cmH₂O, an inspiratory-to-expiratory (I:E) ratio of 1:2, and a respiratory rate (RR) adjusted to maintain an arterial partial pressure of carbon dioxide (PaCO₂) between 35 and 45 mmHg. The fraction of inspired oxygen (FiO₂) was titrated to achieve a peripheral oxygen saturation (SpO₂) between 92% and 96%.
This strategy was maintained during a stabilization period, lasting on average 30 to 120 minutes, defined as the time required for the stabilization of vital signs and vasoactive drug levels, correction of coagulation-related blood factors, and optimization of volemia to achieve an inferior vena cava (IVC) of a minimum diameter of 18 mm.
After this stabilization period, pulmonary mechanics and arterial blood gas variables were collected, and patients were randomly allocated. Subsequently, in the CG, PEEP was increased to 10 cmH₂O, and after 5 minutes at this adjusted PEEP level, new measurements of pulmonary mechanics and arterial blood gases were recorded. Patients were ventilated using this strategy until the spontaneous breathing trial (SBT), which was performed with pressure support of 7 cmH₂O and PEEP of 5 cmH₂O for 30 minutes. The timeline of the research protocol in the immediate postoperative period is represented in Figure1.
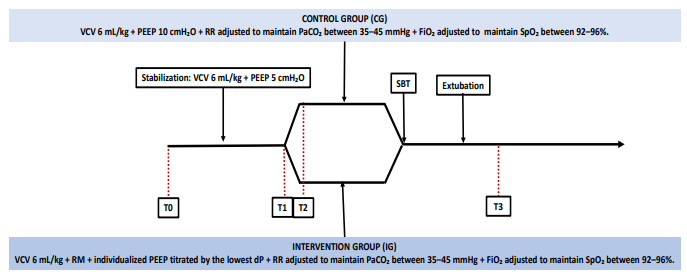
Figure 1:Timeline of the research protocol in the immediate postoperative period
VCV: volume-controlled ventilation; PEEP: positive end-expiratory pressure; RM: recruitment maneuver; RR: respiratory rate; FiO₂: fraction
of inspired oxygen; SpO₂: peripheral oxygen saturation; PaCO₂: arterial carbon dioxide partial pressure; ECOTT: transthoracic echocardiography; CG: control group; IG: intervention group. Time points: T0 : Admission to the ICU and beginning of stabilization (Arterial blood
gas analysis + Transthoracic echocardiography – ECOTT); T1 : Randomization into CG and IG (Pulmonary mechanics assessment); T2 :
Five minutes after PEEP adjustment (Arterial blood gas analysis + Pulmonary mechanics); T3: Sixty minutes after extubation; T4: Hospital
discharge
Intervention group
Patients in the intervention group (IG) were initially admitted to conventional protective mechanical ventilation in the immediate postoperative period (IPP), also in the volume-controlled ventilation (VCV) mode, with a tidal volume (VT) of 6 mL/kg of predicted body weight, a PEEP of 5 cmH₂O, an I:E ratio of 1:2, and an RR adjusted to maintain PaCO₂ between 35 and 45 mmHg. FiO₂ was set to the minimum level required to maintain SpO₂ between 92% and 96%.
This initial strategy was maintained during the stabilization period, lasting on average 30 to 120 minutes, defined as the time required for the stabilization of vital signs and vasoactive drug levels, correction of coagulation-related factors, and volemic adjustment to achieve an IVC diameter of 18 mm.
After stabilization, pulmonary mechanics and arterial blood gas variables were collected, and patients were randomly allocated. Subsequently, the IG underwent an alveolar recruitment maneuver (ARM) performed in pressure-controlled ventilation (PCV) mode, with an inspiratory pressure of 15 cmH₂O, FiO₂ = 100%, RR = 10 breaths/min, I:E ratio of 1:1, and an initial PEEP of 5 cmH₂O.
The incremental phase of the recruitment maneuver consisted of increasing PEEP sequentially to 10, 20, and 35 cmH₂O, with the patient maintained at each PEEP level for 30 seconds. Following this, PEEP was decreased to 20 cmH₂O, and the ventilator mode was switched to volume-controlled ventilation (VCV) with a VT of 6 mL/kg predicted body weight, RR = 15 breaths/min, I:E ratio of 1:2, and FiO₂ = 100%.
Subsequently, PEEP was decreased stepwise by 2 cmH₂O increments down to 6 cmH₂O, with the patient maintained at each PEEP level for 30 seconds. Driving pressure (dP) was calculated at each step using a 2-second inspiratory pause at the end of inspiration after 30 seconds at each PEEP level.
At the end of the recruitment maneuver, PEEP was again increased to 35 cmH₂O for 30 seconds, and PEEP titration was then set at the level corresponding to the lowest dP. The ARM was performed with only 30 seconds at the maximum pressure of the maneuver as illustrated in Figure 2.
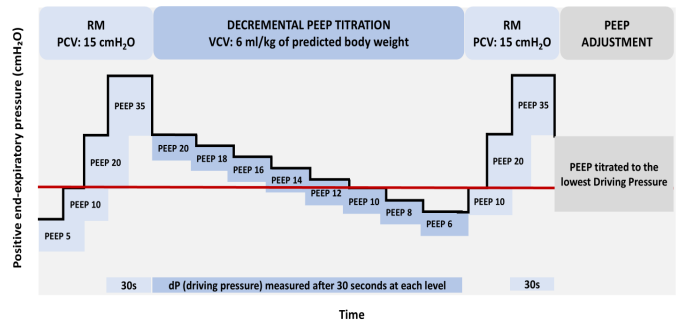
Figure 2:Stepwise alveolar recruitment maneuver followed by decremental PEEP titration and final PEEP adjustment according to the
lowest driving pressure.
PCV: pressure-controlled ventilation; VCV: volume-controlled ventilation; VT: tidal volume; PEEP: positive end-expiratory pressure; RR:
respiratory rate; FiO₂: inspired oxygen fraction; dP: driving pressure
This protocol was applied in the Intervention group to determine the individualized PEEP that minimized the driving pressure (dP), thereby optimizing alveolar recruitment and minimizing both collapse and overdistension. The stepwise recruitment maneuver was followed by decremental PEEP titration, during which dP was measured at each level after 30 seconds of stabilization. The final PEEP was defined as the level corresponding to the lowest dP, ensuring an individualized protective ventilation strategy aimed at improving postoperative pulmonary mechanics and reducing the incidence of PPCs.
Sample size
The sample size was calculated using an online calculator from the Department of Statistics, University of British Columbia (https://www.stat.ubc.ca/~rollin/stats/ssize/b2.html). Based on our previous pilot project and in line with the literature, we estimated an expected incidence of moderate-to-severe postoperative pulmonary complications (PPC ≥ grade 3) of 32% in the control group and 15% in the individualized PEEP group. Assuming a two-sided test, α = 0.05 and power = 80%, the required sample size was 76 patients per group.
The online randomization platform used in the study allowed a maximum of 100 allocations per block; therefore, the first 100 eligible patients were randomized initially. After completion of enrollment of these cases, a post-hoc power analysis demonstrated an achieved statistical power of 89%, confirming a clinically meaningful effect size in favor of the intervention. In addition to reaching the predefined interim enrollment threshold and demonstrating robust statistical significance, continuation of recruitment became operationally unfeasible due to the sustained impact of the COVID-19 and post-COVID periods on hospital workflow, including increased clinical demand, staffing constraints, and limitations in research logistics and data collection. These circumstances, combined with the observed treatment effect, supported an ethically and methodologically justified decision to discontinue further recruitment while preserving trial validity. The study became underpowered for secondary outcomes.
Randomization
Randomization was performed using the software available at https://aurora.shinyapps.io/random_gen/, registered under PIN 270107, with stratification of 100 patients randomly allocated in a 1:1 ratio. After obtaining written informed consent, patients were selected by the HUPE cardiac surgery team, which remained blinded to group allocation.
Each patient was scheduled for surgery according to clinical priorities, considering factors such as case urgency, prosthesis availability (for valve replacement cases), and blood bank readiness for crossmatching. After de procedure, those with a signed informed consent form, who met all inclusion criteria and presented no exclusion criteria where reassessed following a stabilization period. Once deemed eligible, each patient was allocated according to the pre-established randomization sequence.
All analyses were performed according to the per-protocol principle, excluding patients who met predefined interruption criteria (n=3): one in the control group (due to need for rescue alveolar recruitment maneuver) and two in the intervention group (one for bradycardia and hypertension during PEEP titration, and one for hypotension and hemodynamic instability during recruitment maneuver). No imputation of missing data was performed, as these exclusions occurred before outcome assessment. Therefore, the final analysis included 97 patients (49 in the control group and 48 in the intervention group).
This approach was chosen to ensure the accuracy of physiological and outcome comparisons between patients who fully completed the ventilation protocol. Given that the exclusions were strictly due to protocol-defined safety endpoints (hemodynamic instability or oxygenation failure), and not random withdrawal or data loss, the per-protocol analysis provides a more precise assessment of the intervention’s physiological effects while maintaining methodological rigor.
All evaluators (physicians, nurses, and physiotherapists) were blinded to group allocation, except for the research team responsible for performing the recruitment maneuver (ARM) and managing the randomization process.
Statistical analysis
Primary analysis followed per-protocol principles. Categorical variables compared using chi-square tests; continuous variables using Mann-Whitney U. Relative risks, confidence intervals, absolute risk reduction, and number needed to treat were calculated.
Results
Patient flow and study population
During the data collection period (July 2021 to October 2023), 843 cardiac surgeries were performed. After applying the inclusion and exclusion criteria, 743 patients were excluded, leaving 100 patients who were randomized: 50 to the control group (CG) and 50 to the intervention group (IG) as shown in Figure 3.

Figure 3:Study flowchart of patient allocation
TCLE: informed consent form; IVC: inferior vena cava; SPAP: systolic pulmonary artery pressure; CPB: cardiopulmonary bypass;
RIMA: right internal mammary artery; Poi: immediate postoperative period; ARM: alveolar recruitment maneuver
In the CG, one patient was withdrawn because of PaO₂/FiO₂ <150 mmHg after 60 minutes on PEEP 10 cmH₂O, requiring a rescue ARM. In the IG, two patients met discontinuation criteria: one due to hypertension and bradycardia during PEEP titration, and another due to hypotension with hemodynamic instability (MAP <60 mmHg, norepinephrine >2 µg/kg/min). These three patients were excluded from the final analysis.
Baseline characteristics
Table 2 summarizes the baseline characteristics of the patients in both groups. There were no statistically significant differences between the groups regarding demographic or anthropometric variables, confirming homogeneous distribution. Groups were well balanced with no significant differences.
Table 2. Baseline characteristics of patients in the control and intervention groups
| Variables | Control N (%) | Intervention N (%) | p-value |
|---|---|---|---|
| Female | 17 (34.7%) | 21 (43.8%) | 0.361 |
| Male | 32 (65.3%) | 27 (56.3%) | 0.361 |
| Age (years) | 65 (58–68) | 66 (58–72) | 0.196 |
| BMI (kg/m²) | 27 (24–29) | 27 (25–31) | 0.201 |
Values are expressed as n (%) or median (interquartile range). No statistically significant differences were observed between groups.
Intraoperative characteristics
There were no significant differences in surgical types or intraoperative times between groups, as shown in Table 3.
Table 3.Intraoperative characteristics
| Type of Surgery | Control N (%) | Intervention N (%) | p-value |
|---|---|---|---|
| ASD | 1 (2.0%) | 1 (2.1%) | 0.988 |
| CABG | 38 (77.6%) | 34 (70.8%) | 0.449 |
| VR | 8 (16.3%) | 9 (18.8%) | 0.754 |
| CABG + VR | 2 (4.1%) | 3 (6.3%) | 0.629 |
| PLASTY | 0 (0.0%) | 1 (2.1%) | 0.310 |
| CPB time (min) | 85 (73–99) | 85 (66–112) | 0.988 |
| Aortic cross-clamp time (min) | 74 (20–80) | 66 (58–83) | 0.694 |
Table 4.Initial Ventilatory Parameters
| Ventilatory Data | Control | Intervention | p-value |
|---|---|---|---|
| VT (mL) | 370 (300–400) | 375 (320–400) | 0.361 |
| VT / Predicted Body Weight (mL/kg) | 6.03 (5.96–6.06) | 6.03 (5.99–6.06) | 0.186 |
| dP (cmH₂O) | 9.00 (7–10) | 9.00 (8–11) | 0.221 |
| Cst (mL/cmH₂O) | 44.44 (32.00–57.14) | 40.45 (36.25–48.65) | 0.355 |
| PaO₂/FiO₂ | 285 (208–382) | 347 (249.5–381) | 0.500 |
Values are expressed as median (interquartile range). No statistically significant differences were observed between group. VT: tidal volume; dP: driving pressure; Cst : static compliance; PaO₂/FiO₂: arterial oxygen partial pressure to inspired oxygen fraction ratio.
Values are expressed as n (%) or median (interquartile range). No statistically significant differences were observed between groups. ASD: atrial septal defect; CABG: coronary artery bypass grafting; VR: valve replacement; PLASTY: valvuloplasty or cardiac reconstructive procedure; CPB: cardiopulmonary bypass; CLAMP: aortic cross-clamping.
Outcomes
All patients were followed daily by a multidisciplinary team consisting of physicians, physiotherapists, nurses, nutritionists, and psychologists. Each patient underwent a comprehensive clinical evaluation, including laboratory and imaging studies such as chest ultrasonography, chest X-ray, and, when clinically indicated, chest computed tomography (CT). Chest radiographs were routinely performed on the first and second postoperative days and at the time of ICU discharge, with additional imaging obtained as clinically necessary.
The interpretation of clinical, laboratory, and imaging findings, as well as the classification of postoperative pulmonary complications (PPCs), was conducted independently by two experienced intensive care physiotherapists, both blinded to group allocation. Only concordant evaluations between the two assessors were accepted for scoring, and any discrepancies were resolved by consensus.
Patients were followed daily until hospital discharge, and the worst PPC grade observed during hospitalization was recorded. PPCs were classified according to the modified Kroenke scale, adapted from Costa Leme et al. (2), as shown below. Complications of grade ≥3 were considered clinically significant and defined the primary outcome of the study. Post-intervention results, presented in Table 5, demonstrate significant differences between the Control and Intervention groups regarding respiratory parameters and clinical outcomes.
Table 5.Post-Intervention Respiratory and Clinical Outcomes
| Variables | Control | Intervention | p-value |
|---|---|---|---|
| PEEP (cmH₂O) | 10 (10–10) | 8 (6–10) | < 0.001* |
| dP (cmH₂O) | 8 (7–11) | 6 (5–7) | < 0.001* |
| Cst (mL/cmH₂O) | 41 (33–51) | 53 (47–66) | < 0.001* |
| PaO₂/FiO₂ | 377 (289–410) | 472 (388–571) | < 0.001* |
| Duration of mechanical ventilation (min) | 275 (235–445) | 420 (339–498) | 0.003* |
| ICU length of stay (days) | 4 (3–5) | 4 (3–5) | 0.899 |
Values are expressed as median (interquartile range). Statistically significant differences were observed in PEEP, driving pressure (dP), static compliance (Cst), PaO₂/FiO₂ ratio, and duration of mechanical ventilation, favoring the intervention group. No significant difference was found in ICU length of stay between groups. PEEP : positive end-expiratory pressure; dP: driving pressure; Cst: static compliance; PaO₂/FiO₂ : arterial oxygen partial pressure to inspired oxygen fraction ratio; ICU: intensive care unit.
The Intervention group showed significantly lower PEEP values, with a median of 8 cmH₂O (interquartile range: 6–10), compared with 10 cmH₂O (10–10) in the Control group (p < 0.001). Similarly, driving pressure (dP) was lower in the Intervention group, with median values of 6 cmH₂O (5–7), compared with 8 cmH₂O (7–11) in the Control group (p < 0.001), indicating a reduced ventilatory load.
Static respiratory system compliance (Cst) also showed a significant improvement in the Intervention group, with a median of 53 mL/cmH₂O (47–66), compared with 41 mL/cmH₂O (33–51) in the Control group (p < 0.001). Furthermore, the PaO₂/FiO₂ ratio was significantly higher in the Intervention group, with values of 472 (388–571) compared with 377 (289–410) in the Control group (p < 0.001), suggesting enhanced oxygenation in patients who received the individualized intervention.
Regarding the duration of mechanical ventilation, a significant increase was observed in the Intervention group, with a median of 420 minutes (339–498), compared with 275 minutes (235–445) in the Control group (p = 0.003). However, no significant difference was found in ICU length of stay, as both groups presented a median of 4 days (3–5) (p = 0.899).
Primary outcome - postoperative pulmonary complications (PPCs ≥3)
The incidence of PPCs ≥ 3 was 40.8% in the Control group compared with 12.5% in the Intervention group, representing a 69.4% reduction in the Intervention group (RR 3.27; 95% CI 1.56–6.82; p = 0.002). Absolute risk reduction 28.3%, corresponding to a number needed to treat (NNT) of 4, as shown in Table 6.
Table 6.Incidence of PPCs ≥ 3 and Pneumonia
| Variable | Control N (%) | Intervention N (%) | Relative Risk (95% CI) | p-value |
|---|---|---|---|---|
| Pneumonia | 14 (28.6%) | 4 (8.3%) | 3.43 (1.34 to 8.80) | 0.010* |
| CPPs ≥ 3 | 20 (40.8%) | 6 (12.5%) | 3.27 (1.56 to 6.82) | 0.002* |
Values are expressed as n (%). Statistical significance was determined using the chi-square test. PPCs – postoperative pulmonary complications.
Secondary outcomes
Regarding secondary outcomes, the incidence of pneumonia was 70.7% lower in the Intervention Group (IG) compared with the Control Group (CG) (8.3% vs. 28.6%; p = 0.010; RR 3.43, 95% CI 1.34–8.80). dP significantly decreased (6 vs 8 cmH₂O, p < 0.001). PaO₂/FiO₂ improved and compliance increased. No cases of barotrauma, pneumothorax, or protocol-related reintubations were observed. In addition, no severe arrhythmias occurred in either group during the postoperative period. The median ICU length of stay was 4 days in both groups (p = 0.899). Hospital mortality up to discharge was 2.1% in the Intervention Group and 6.1% in the Control Group (p = 0.317).
Ventilatory mechanics and driving pressure
The maintenance of reduced pulmonary pressures after the recruitment maneuver (ARM) emerges as a relevant strategy for preventing pneumonia in the immediate postoperative period following cardiac surgery, as evidenced by the findings of this study and illustrated in Figure 4.
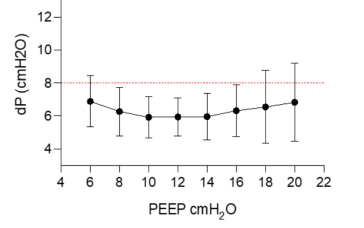
Figure 4:Effect of the recruitment maneuver on driving pressure (dP). PEEP: positive end-expiratory pressure; dP : driving pressure (alveolar distending pressure).
The intervention group showed a significant reduction in dP after ARM and PEEP titration (6 cmH₂O vs. 8 cmH₂O; p < 0.001). Lower dP values were associated with better PaO₂/FiO₂ ratios (472 vs. 377; p < 0.001), suggesting improved lung recruitment and oxygenation. The maintenance of lower pulmonary pressures after ARM was a relevant strategy for pneumonia prevention in the immediate postoperative period.
PEEP individualization
Among the 48 patients in the intervention group, 72% (n=35) had an optimal PEEP ≤10 cmH₂O, equivalent to the hospital’s standard PEEP setting.
The Figure 5 presented above highlights the relevance of individualized PEEP in optimizing postoperative respiratory mechanics. In panel A of Figure 5, the dispersion of individualized PEEP values can be observed, demonstrating that a fixed approach—whether the 10 cmH₂O PEEP used in the Control group or the 13 cmH₂O PEEP applied in the protocol by Costa Leme et al. [2], does not account for interindividual variability in pulmonary mechanics. Consequently, a considerable number of patients receive PEEP levels either higher or lower than those required to minimize driving pressure (dP). Panel B illustrates the frequency or number of times that a given PEEP level represented the PEEP corresponding to the lowest dP. This graph shows that as PEEP increases, the likelihood of that PEEP being the level with the lowest dP decreases, reinforcing that a decremental PEEP titration strategy is essential to avoid excessive pressures that may result in pulmonary overdistension.
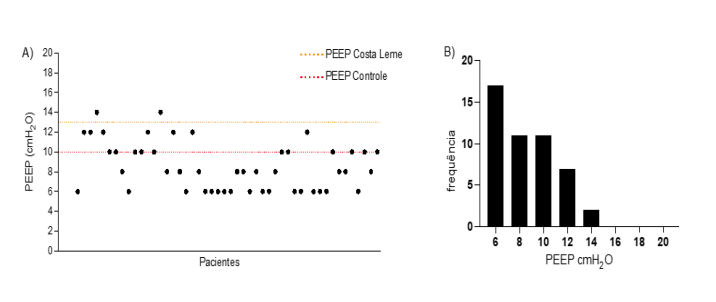
Figure 5:Distribution of individualized PEEP values after ARM.
Individual PEEP distribution compared with fixed PEEP 10 cmH₂O. A) Individualized PEEP of all patients in the Intervention group
after the ARM compared with the PEEP of 13 cmH₂O reported by Costa Leme and the PEEP of 10 cmH₂O used in the Control group.
B) Frequency or number of times in which that PEEP level represented the PEEP with the lowest dP. PEEP: Positive end-expiratory
pressure.
Table 7.Description of PPCs ≥ 3 Between Groups
| Variable | Control N (%) | Intervention N (%) | Relative Risk (95% CI) | p-value |
|---|---|---|---|---|
| Pneumonia | 14 (28.6%) | 4 (8.3%) | 3.43 (1.34 to 8.80) | 0.010* |
| Reoperation | 2 (4.1%) | 3 (6.3%) | 0.65 (0.12 to 3.68) | 0.629 |
| Pneumothorax | 2 (4.1%) | 0 (0.0%) | – | 0.157 |
| Prolonged MV | 2 (4.1%) | 0 (0.0%) | – | 0.157 |
| Reintubation < 48h | 0 (0.0%) | 1 (2.1%) | – | 0.310 |
| Pleural effusion | 1 (2.0%) | 0 (0.0%) | – | 0.320 |
| Death | 3 (6.1%) | 1 (2.1%) | 2.94 (0.36 to 24.30) | 0.317 |
PPCs: postoperative pulmonary complications; MV: mechanical ventilation. Values are expressed as n (%).
Complications and adverse events
No patient in the intervention group developed barotrauma, pneumothorax, or prolonged mechanical ventilation. Only one reintubation (<48 h) was observed in the IG due to transient airway obstruction (“tongue drop”), resolved without sequelae. One pleural effusion requiring drainage occurred in the CG (2.0%; p = 0.320). No reoperation difference was observed (4.1% CG vs. 6.3% IG; p = 0.629).
Discussion
The incidence of PPCs ≥ 3 was 40.8% in the Control group versus 12.5% in the Intervention group, resulting in a 69.4% reduction in the Intervention group (p = 0.002), with a relative risk (RR) of 3.27 (95% CI: 1.56–6.82) and an absolute reduction of 28.3%. The incidence of pneumonia was 70.7% lower in the Intervention group (8.3%) compared with the Control group (28.6%, p = 0.010), with an RR of 3.43 (95% CI: 1.34–8.80).
The choice to analyse PPCs of grade ≥ 3 as a relevant outcome was based on the significant clinical impact of these complications on patient progression, since a score ≥ 3 includes severe events such as pneumonia, prolonged non-invasive ventilation, reintubation, invasive mechanical ventilation lasting more than 48 hours, and pleural effusion requiring drainage. These complications are associated with higher morbidity, prolonged need for ventilatory support, longer ICU and hospital stays, and potential implications for mortality.
The recruitment maneuver (ARM) followed by individualized PEEP titration enabled the Intervention group to achieve significantly lower median dP values (6.0 cmH₂O vs. 8.0 cmH₂O; p < 0.001), reinforcing the hypothesis that reducing driving pressure is directly associated with pulmonary protection. In patients from the Intervention group, both mean and median dP remained at 6 cmH₂O within the PEEP range of 8-16 cmH₂O. This finding suggests that, from the standpoint of lung protection, any PEEP level within this range would ensure the lowest dP. However, considering the hemodynamic effects of PEEP, selecting the lowest value within this range is physiologically reasonable. Moreover, only two patients required PEEP levels above 13 cmH₂O, suggesting that the PEEP adopted by Costa Leme et al. may have been excessive, not only in terms of pulmonary protection but also hemodynamic optimization.
The variation in dP across different PEEP levels highlighted the challenge of defining a universal setting that optimizes respiratory mechanics homogeneously. In this study, individualized PEEP titration enabled the minimization of dP in a personalized manner, promoting alveolar optimization, preventing both collapse and hyperinflation, and reducing shear stress without compromising cardiovascular stability.
The “Open Lung Concept (OLC)” proposed by Lachmann [25] supports this exact principle: recruiting collapsed alveoli and setting PEEP to avoid both atelectasis and alveolar overdistension. Consequently, applying a fixed PEEP, even after recruitment, may result in excessive pressures for some patients and inadequate pressures for others. Ventilatory strategies based on this concept can minimize right ventricular overload without compromising respiratory mechanics [12], contributing to better hemodynamic stability, reduced need for vasopressors, and fewer adverse postoperative effects.
Additionally, individualizing PEEP based on the lowest dP, using values lower than those recommended in previous protocols, may have reduced the hemodynamic impact of ventilation. One of the effects of PEEP is the decrease in the venous return pressure gradient and the increase in right atrial pressure, which can reduce right and left ventricular preload, decrease left ventricular afterload, and increase right ventricular afterload, potentially leading to right ventricular failure in the long term [26]. However, further studies are required to determine the true magnitude of vasopressor reduction after ARM in patients with optimized volemia in the immediate postoperative period of cardiac surgery.
The ARM combined with individualized PEEP not only significantly reduced dP but also improved the PaO₂/FiO₂ ratio (472 vs. 377, p < 0.001), thereby enabling reduced oxygen consumption in the Intervention group.
Preclinical studies have demonstrated that atelectasis not only reduces pulmonary compliance and impairs gas exchange but also triggers a “double-hit phenomenon,” in which regional hypoventilation associated with alveolar collapse activates cytokine-mediated inflammatory pathways, promoting the development of pneumonia [27,28].
Furthermore, mechanical ventilation with high pressures and without adequate ARM leads to markedly elevated levels of tumor necrosis factor-alpha (TNF-α) in bronchoalveolar fluid, which is associated with greater pulmonary inflammation and increased risk of respiratory failure. TNF-α also enhances the activation of other inflammatory cytokines, including interleukin-6 (IL-6) and interleukin-8 (IL-8), amplifying lung injury and increasing the risk of infectious complications [29].
TNF-α is one of the key mediators of pulmonary and systemic inflammatory responses, released mainly by alveolar macrophages and epithelial cells in response to mechanical stress caused by high dP and persistent atelectasis. This factor increases alveolar-capillary barrier permeability, contributing to pulmonary edema and facilitating bacterial translocation, thereby making the lung more susceptible to opportunistic infections such as postoperative pneumonia [29].
IL-6, in turn, is a pro-inflammatory cytokine widely studied in pulmonary inflammatory responses, particularly in mechanical ventilation and ARDS. It plays a central role in inflammatory mechanotransduction, acting as a sensitive biomarker of the degree of VILI and a key mediator in the development of complications such as pneumonia and pulmonary fibrosis. Preclinical studies demonstrate that ventilation with high dP and without adequate alveolar recruitment results in marked increases in IL-6 levels in pulmonary fluids and plasma, reflecting greater mechanical stress and enhancing systemic inflammation [29].
Experimental models of VILI have shown that tolerance to atelectasis is associated with increased expression of these interleukins, exacerbating pulmonary inflammation and predisposing to secondary infection [29,30]. Moreover, the concept of alveolar recruitment followed by decremental PEEP titration is physiologically supported by evidence showing that this approach reduces ventilation heterogeneity, minimizes mechanical overload of still-aerated lung units, and preserves alveolar epithelial integrity, thereby preventing the development of pneumonia [31].
The findings of this clinical trial corroborate the pathophysiological concept of biotrauma, as the reduction of dP in the Intervention group was associated with a significantly lower incidence of pneumonia (8.3% vs. 28.6%, p = 0.010), reinforcing the need for ventilatory strategies that minimize mechanical stress and inflammatory mechanotransduction. This is consistent with recent meta-analyses demonstrating that individualized PEEP reduces pulmonary inflammation and improves oxygenation without compromising hemodynamic stability [20].
The Intervention group showed no cases of pneumothorax or prolonged mechanical ventilation, whereas in the Control group the incidence of these complications was 4.1% (p = 0.157). Although the intervention group showed longer duration of mechanical ventilation, this finding may reflect a more protective ventilatory strategy and stricter extubation criteria rather than worse clinical evolution. Importantly, the longer duration of mechanical ventilation did not translate into worse clinical outcomes, as ICU length of stay and complication rates remained similar or improved.
The need for reoperation was similar between groups, occurring in 4.1% of Control and 6.3% of Intervention patients (RR: 0.65; 95% CI: 0.12–3.68; p = 0.629). These findings suggest that the protocol did not significantly influence complications requiring additional surgical interventions, consistent with the findings of Costa Leme et al.
The incidence of reintubation within 48 hours and pleural effusion was low in both groups, with no statistically significant differences. In the Intervention group, there was one case of reintubation (2.1%; p = 0.310) due to tongue drop, characterized by posterior displacement of the tongue compromising airway patency. Orotracheal extubation was successfully performed four hours later, without complications. Similarly, in the Control group, one case of pleural effusion requiring drainage occurred, representing 2.0% of patients (p = 0.320).
Additionally, the proposed ventilation strategy did not increase serious adverse events. Hospital mortality was low in both groups, showing a decreasing trend in the Intervention group (2.1% vs. 6.1%), although without statistical significance (p = 0.317). These findings are consistent with Costa Leme et al. (2017), who also reported reduced hospital mortality (2.5% in the intensive group vs. 4.9% in the moderate group), with a non-significant difference of −2.4% (p = 0.27).
These data suggest that while the new protocol provided benefits regarding pulmonary complications, its impact on mortality may be less pronounced or may require longer follow-up. The RR of 2.94 in the Intervention group and 95% CI of 0.36–24.3 broaden the uncertainty about the clinical relevance of this difference. Other factors such as the severity of patients’ preoperative clinical conditions, comorbidities, surgical wait time, and preoperative hospital stay may influence mortality, indicating that further studies are necessary to determine the long-term effectiveness of the proposed protocol.
Regarding ICU length of stay, there was no significant difference between groups, with a median of four days for both. This finding may reflect the effectiveness of the ventilatory strategy in improving pulmonary mechanics and reducing PPCs without substantially affecting ICU recovery time. It is also important to consider the specific context of the cardiac surgery unit at HUPE, which has only 12 ICU beds to accommodate an average of 12 cardiac surgeries per week. In this setting, hospital discharge ideally between the third and fifth postoperative day is crucial to ensure bed turnover necessary to meet the surgical target, especially given the long waiting list of critically ill patients requiring surgery through the Brazilian Unified Health System (SUS). Therefore, ventilatory strategies that maintain a median ICU stay around four days or less—without compromising patient safety and optimizing clinical outcomes-may significantly contribute to service efficiency and broaden access for other individuals awaiting surgical procedures.
Our findings align with meta-analytic evidence that recruitment maneuvers, when brief and followed by individualized PEEP, can improve lung aeration and reduce postoperative pulmonary complications in cardiac surgery cohorts. The divergent outcomes reported in ARDS trials [32] underline that population characteristics and ARM technique (duration, pressure, monitoring) fundamentally modify the benefit-risk balance; in elective cardiac surgery our protocol used short, monitored inflations and titrated PEEP to minimize driving pressure, which plausibly explains the favourable safety and efficacy profile observed. Future multicenter studies should standardize ARM protocols and evaluate ultrasound or driving pressure guided approaches to optimize patient selection and safety.
This randomized clinical trial demonstrates that individualized PEEP titration guided by driving pressure significantly reduces clinically relevant PPCs after cardiac surgery. The magnitude of benefit suggests a strong physiological effect, likely mediated by reduced lung stress, improved alveolar recruitment, and decreased inflammatory activation.
The findings are consistent with the open-lung concept and prior evidence linking lower driving pressure to improved outcomes. Unlike high-pressure recruitment protocols, our short and monitored maneuver minimized hemodynamic impact.
Although ICU length of stay was not reduced, this may reflect institutional logistics and bed turnover requirements rather than lack of clinical benefit.
Study limitations
This was a single-center trial with a modest sample size (n=100), which may limit generalizability. The absence of advanced monitoring tools such as transpulmonary pressure or electrical impedance tomography precluded detailed assessment of regional ventilation. Nonetheless, the homogeneity of the sample, rigorous blinding of evaluators, and consistent protocol adherence strengthen the reliability of the results.
Future multicenter studies are warranted to confirm these findings and to explore whether ΔP-guided PEEP titration can reduce not only PPCs but also long-term morbidity and healthcare costs in broader cardiac surgical populations.
Clinical implications
Driving pressure-guided PEEP titration represents a simple bedside strategy with potential to improve postoperative outcomes.
Conclusion
This randomized controlled trial demonstrated that a lung-protective ventilation strategy combining an alveolar recruitment maneuver followed by individualized PEEP titration based on the lowest driving pressure significantly reduced postoperative pulmonary complications and pneumonia after elective cardiac surgery.
Unlike previous high-pressure or fixed-PEEP protocols, this approach achieved pulmonary protection without compromising hemodynamic stability.
Individualized PEEP titration guided by dP represents a simple, physiologically sound, and safe bedside method that may be incorporated into postoperative care to enhance outcomes and reduce morbidity in cardiac surgery patients. These findings support ΔP-guided PEEP titration as a clinically applicable, physiologically grounded strategy that significantly reduces severe PPCs in cardiac surgery.
Abbreviations
ARDS: Acute respiratory distress syndrome; ARM: Alveolar recruitment maneuver; ASD: Atrial septal defect; BMI: Body mass index; CABG, Coronary artery bypass grafting; CLAMP, Aortic cross-clamping; CPAP, Continuous positive airway pressure; CPB, Cardiopulmonary bypass; Cst, Static compliance; dP, Driving pressure; ΔdP, Percentage change in driving pressure; FRC, Functional residual capacity; HUPE, Pedro Ernesto University Hospital; ICF, Informed consent form; ICU, Intensive care unit; IL-6, Interleukin-6; IL-8, Interleukin-8; IVC, Inferior vena cava; MAP, Mean arterial pressure; MV, Mechanical ventilation; OLC, Open lung concept; OTI, Orotracheal intubation; PaCO₂, Arterial partial pressure of carbon dioxide; PaO₂/FiO₂, Ratio of arterial oxygen partial pressure to inspired oxygen fraction; PAH, Pulmonary arterial hypertension; PEEP, Positive end-expiratory pressure; PPCs, Postoperative pulmonary complications; Ppeak, Peak inspiratory pressure; Pplat, Plateau pressure; RF, Respiratory failure; RIMA, Right internal mammary artery; SBPT, Brazilian Thoracic Society; SBT, Spontaneous breathing trial; SpO₂, Peripheral oxygen saturation; sPAP, Systolic pulmonary artery pressure ; SUS, Brazilian Unified Health System; TNF-α: Tumor necrosis factor alpha; UERJ: Rio de Janeiro State University; VILI: Ventilator-induced lung injury; VT: Tidal volume
Trial Registration
ReBEC – RBR-2nmwxwt
Funding
No external funding
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Tanner TG, Colvin MO. Pulmonary complications of cardiac surgery. Lung. 2020;198(6):889-896. doi:10.1007/s00408-020-00405-7.
2. Costa Leme A, Hajjar LA, Volpe MS, Fukushima JT, De Santis Santiago RR, Osawa EA, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications: a randomized clinical trial. JAMA. 2017;317(14):1422-1432.
3. Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-1350.
4. Neto AS, Hemmes SNT, Barbas CSV, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med. 2016;4(4):272-280.
5. Lawrence VA, John MAJ. Operative risk in patients with severe obstructive pulmonary disease. 2015.
6. Ball L, Costantino F, Pelosi P. Postoperative complications of patients undergoing cardiac surgery. Curr Opin Crit Care. 2016;22(4):386-392.
7. Reber A, Budmiger B, Wenk M, Haefeli WE, Wolff T, Bein T, et al. Inspired oxygen fraction after cardiopulmonary bypass: effects on pulmonary function with regard to endothelin-1 concentrations and venous admixture. Br J Anaesth. 2000;84(5):565-570.
8. Allou N, Bronchard R, Guglielminotti J, Dilly MP, Provenchere S, Lucet JC, et al. Risk factors for postoperative pneumonia after cardiac surgery and development of a preoperative risk score. Crit Care Med. 2014;42(5):1150-1156.
9. Laffey JG, Boylan JF, Cheng DCH. The systemic inflammatory response to cardiac surgery. Anesthesiology. 2002;97(1):215-252.
10. Magnusson L, Spahn DR. Atelectasis is a major cause of hypoxemia and shunt after cardiopulmonary bypass. Anesthesiology. 1997;87(5):1153-1163.
11. Zupancich E, Paparella D, Turani F, Munch C. Effects of ventilation strategy during cardiac surgery: a randomized clinical trial. 2005.
12. Miranda DR, Gommers D, Struijs A, Meeder H, Schepp R, Hop W, et al. The open lung concept: effects on right ventricular afterload after cardiac surgery. Br J Anaesth. 2004;93(3):327-332.
13. Pelosi P, Ball L. Should we titrate ventilation based on driving pressure? Intensive Care Med. 2018;44(7):1171-1173.
14. Amato MBP, Meade MO, Slutsky AS, Brochard L, Costa ELV, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747-755.
15. Bugedo G, Retamal J, Bruhn A. Driving pressure: a marker of severity, a safety limit, or a goal for mechanical ventilation? Crit Care. 2017;21:199.
16. Guérin C, Papazian L, Reignier J, Ayzac L, Loundou A, Forel JM. Effect of driving pressure on mortality in ARDS patients during lung protective mechanical ventilation in two randomized controlled trials. Crit Care. 2016;20(1):384.
17. Hess DR, Kondili D, Burns E, Bittner EA, Schmidt UH. A 5-year observational study of lung-protective ventilation in the operating room: a single-center experience. J Crit Care. 2013;28(4):533.e9-533.e15.
18. Jaber S, Coisel Y, Chanques G, Futier E, Constantin JM, Michelet P, et al. A multicentre observational study of intra-operative ventilatory management during general anaesthesia: tidal volumes and relation to body weight. Anaesthesia. 2012;67(9):999-1008.
19. Young CC, Harris EM, Vacchiano C, Bodnar S, Bukowy B, Elliott RRD, et al. Lung-protective ventilation for the surgical patient: international expert panel-based consensus recommendations. Br J Anaesth. 2019;123(6):898-913.
20. Hu MC, Yang YL, Chen TT, Lee CI, Tam KW. Recruitment maneuvers to reduce pulmonary atelectasis after cardiac surgery: a meta-analysis of randomized trials. J Thorac Cardiovasc Surg. 2022;164(1):171-181.e4.
21. Gattinoni L, Collino F, Camporota L. Mechanical power: meaning, uses and limitations. Intensive Care Med. 2023;49(4):465-467.
22. Cornejo RA, Arellano DH, Ruiz-Rudolph P, Guiñez DV, Morais CCA, Gajardo AIJ, et al. Inflammatory biomarkers and pendelluft magnitude in ARDS patients transitioning from controlled to partial support ventilation. Sci Rep. 2022;12(1):1-9.
23. Dianti J, Fard S, Wong J, Chan TCY, Del Sorbo L, Fan E, et al. Strategies for lung- and diaphragm-protective ventilation in acute hypoxemic respiratory failure: a physiological trial. Crit Care. 2022;26(1):1-10.
24. Silva PL, Ball L, Rocco PRM, Pelosi P. Physiological and pathophysiological consequences of mechanical ventilation. Semin Respir Crit Care Med. 2022;43(3):321-334.
25. Lachmann B. Open up the lung and keep the lung open. Intensive Care Med. 1992;18(6):319-321.
26. Jozwiak M, Teboul JL. Heart–lung interactions: the basics and clinical implications. Ann Intensive Care. 2024;14(1).
27. Gattinoni L, Carlesso E, Caironi P. Stress and strain within the lung. Curr Opin Crit Care. 2012;18(1):42-47.
28. Pelosi P, Rocco PR. Effects of mechanical ventilation on the extracellular matrix. Intensive Care Med. 2008;34(4):631-639.
29. Cabrera-Benítez NE, Laffey JG, Parotto M, et al. Mechanical ventilation-associated lung fibrosis in acute respiratory distress syndrome. Anesthesiology. 2014;121(1):189-198.
30. Cabrera-Benítez NE, Parotto M, Post M. Mechanical stress induces lung fibrosis by epithelial-mesenchymal transition. Intensive Care Med. 2016;40(2):510-517.
31. Kollisch-Singule M, Emr B, Jain SV, Andrews P, Satalin J, Liu J, et al. Effects of airway pressure release ventilation on respiratory mechanics in extrapulmonary lung injury. Intensive Care Med Exp. 2015;3(1):1-13.
32. Cavalcanti AB, Suzumura EA, Laranjeira LN, Paisani DM, Damiani LP, Guimarães HP, et al. Effect of lung recruitment and titrated positive end-expiratory pressure vs low PEEP on mortality in ARDS: a randomized clinical trial. JAMA. 2017;318(14):1335-1345.
Received:February 25, 2026;
Accepted: March 17, 2026;
Published: March 22, 2026.
To cite this article : Lages NC de L, Ávila MB de, Xavier TBDC, Camilo LM. Individualized PEEP Titration Guided by Driving Pressure after Recruitment Maneuver Reduces Postoperative Pulmonary Complications in Cardiac Surgery: A Randomized Controlled Trial. Eur J Respir Med. 2026; 8(1): 487- 498. doi: 10.31488/EJRM.156.
© The Author(s) 2026. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).